Washington University Emergency Medicine Journal Club – August 2025
Dr. Brian Cohn
This month we will be looking at the use of the HINTS exam and Sudbury score to diffferentiate central from peripheral causes of vertigo in the emergency department. For a detailed video demonstrating the HINTS exam please click here. For the previous journal club discussion on the HINTS exam click here.
The PGY-1 article will be appraised using the Diagnostic Test form; the PGY-2 article will be appraised using the Meta-Analysis form; the PGY-3 and PGY-4 articles will be appraised using the Clinical Decision Rule form.
Vignette
While moonlighting in a small, community hospital one evening, you are presented with a 58-year-old gentleman complaining of vertigo. He was at home eating dinner 5 hours prior to arrival when he felt the room begin to suddenly, and violently, spin around him. He notes “I haven’t felt like this since college!” He reports becoming nauseated and vomited several times before “staggering” to his bed where he laid down and tried to “wait it out.” After several hours of constant vertigo, he attempted to get up to go to the bathroom and fell to the floor. The vertigo has been constant, is worse with any change in head position, and is associated with nausea and imbalance. He denies recent URI symptoms, hearing changes, focal weakness or numbness, or speech changes. His past medical history includes hypertension and diabetes, controlled with amlodipine and Maunjaro. On exam he has horizontal beating nystagmus with leftward gaze. Cerebellar exam – including finger to nose, heel to shin, and rapid alternating movements ‐ is otherwise normal. He has an abnormal Romberg’s and is unable to stand or ambulate unassisted. The remainder of his neurologic exam is normal. Head CT, ECG, and labs are all normal. CTA reveals no large vessel occlusion.
Your differential includes two main concerns: either the patient has vestibular neuritis and should be treated symptomatically and discharged, or he has suffered a cerebellar stroke and requires transfer to a hospital with neurology consultation and MRI available. When the patient does not improve after receiving oral meclezine and IV diazepam, you bite the bullet and transfer him to Barnes-Jewish Hospital for further evaluation by the stroke team. On your way home the next morning, you begin wondering if there are any aspects of the history or physical exam that can differentiate between peripheral and central causes of vertigo. A quick search of the literature identifies a Sudbury Vertigo Risk Score, and something referred to as the HINTS exam. You begin delving deeper to determine if either of these could have helped to avoid a hospital transfer…
PICO Question
Population: Adults with new–onset, acute vertigo with otherwise non-focal
neurologic exam
Intervention: Bedside oculomotor testing (HINTS exam) and the Sudbury Vertigo
Risk score
Comparison: MRI, discharge diagnosis, follow-up diagnosis
Outcome: Diagnostic accuracy, morbidity or mortality related to misdiagnosis
Article 1: Dmitriew C, Regis A, Bodunde O, Lepage R, Turgeon Z, McIsaac S, Ohle R. Diagnostic Accuracy of the HINTS Exam in an Emergency Department: A Retrospective Chart Review. Acad Emerg Med. 2021 Apr;28(4):387-393. doi: 10.1111/acem.14171. Epub 2020 Dec 4. PMID: 33171003. [Answer Key]
Article 2: Ohle R, Montpellier RA, Marchadier V, Wharton A, McIsaac S, Anderson M, Savage D. Can Emergency Physicians Accurately Rule Out a Central Cause of Vertigo Using the HINTS Examination? A Systematic Review and Meta-analysis. Acad Emerg Med. 2020 Sep;27(9):887-896. doi: 10.1111/acem.13960. Epub 2020 Apr 8. PMID: 32167642. [Answer Key]
Article 3: Ohle R, Savage DW, Roy D, McIsaac S, Singh R, Lelli D, Tse D, Johns P, Yadav K, Perry JJ. Development of a Clinical Risk Score to Risk Stratify for a Serious Cause of Vertigo in Patients Presenting to the Emergency Department. Ann Emerg Med. 2025 Feb;85(2):122-131. doi: 10.1016/j.annemergmed.2024.06.003. Epub 2024 Aug 1. PMID: 39093245. [Answer Key]
Article 4: van Patot ET, Roy D, Baraku E, Patel K, McIsaac S, Singh R, Lelli D, Tse D, Johns P, Yadav K, Savage DW, Perry JJ, Ohle R. Validation of the Sudbury Vertigo Risk Score to risk stratify for a serious cause of vertigo. Acad Emerg Med. 2025 Aug;32(8):863-873. doi: 10.1111/acem.70017. Epub 2025 Mar 11. PMID: 40070159; PMCID: PMC12352473. [Answer Key]
Bottom Line
Acute dizziness remains among the more challenging presentations for emergency
physicians. While many patients present with benign, though often debilitating,
peripheral causes of dizziness (BPPV, vestibular neuritis), differentiating these from
more concerning central causes can be difficult. While the HINTS exam—a bedside
assessment consisting of 3 physical exam findings—demonstrated a high degree of
accuracy in differentiating central from peripheral causes of vertigo, initial studies
employed neuro-otologists, neuro-ophthalmologists, and neurologists undergoing
specific study training prior to evaluating the test.
A recent retrospective analysis of data from a tertiary care center in Ontario, CA,
found that when used by emergency physicians without specific training, the HINTS
exam is much more problematic. The HINTS exam was used in 450 patients over a 4
year period, but was found to be appropriate to use in only 15 cases (3.1%). The test
demonstrated a specificity of 95% (95% CI 94 to 98) owing to the low incidence of a
central cause, but had a sensitivity of 0% (95% CI o to 39).
A meta-analysis published prior to this retrospective study found equally concerning
results. The pooled sensitivity and specificity of the HINTS examination were 96.7%
(95% CI 93.1 to 98.5) and 94.8% (95% CI 91 to 97.1) for neurologists/neuroophthalmologists
(LR+ 18.6 and LR- 0.03). In a single study including both emergency physicians and neurologists, the sensitivity and specificity were only 83.3% and 43.8% (LR+ 1.48 and LR- 0.38). While it was not possible to differentiate those performing the exam in this study, there was no specific training in the use of the HINTS exam prior to study initiation. While this evidence does not preclude the use of the HINTS exam by emergency physicians, it does suggest the need for specific training in its use prior to integration into clinical practice.
More recently, a clinical decision rule (CDR) called the Sudbury Vertigo Risk Score
was derived and retrospectively validated to help differentiate central from
peripheral causes of vertigo in the emergency department (Table 2). In the
derivation cohort of patients presenting to one of 3 urban Canadian tertiary care
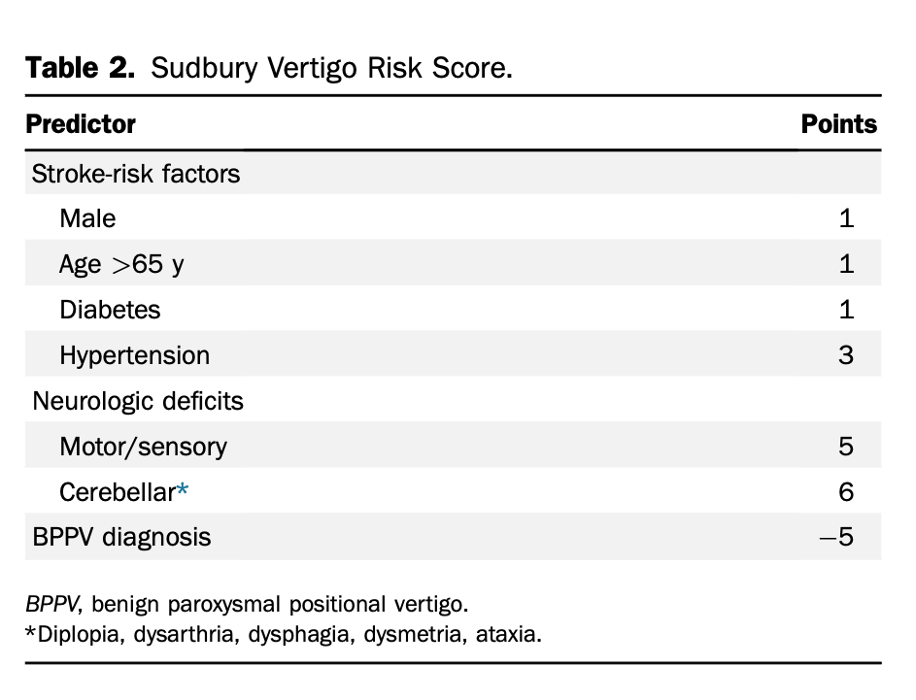
teaching hospitals (n = 2078), the sensitivity was 100% (95% CI 97-100%) and the
specificity was 72.1% (95% CI 70.1% to 74%) for a score >4, corresponding to a LRof
0 and LR+ of 3.58. The score was then retrospectively validated in a cohort of
patients who had presented to the same emergency departments over a time period
preceding the derivation study (n = 4559). Using the same cutoff, the sensitivity was
100% (95% CI 96.5% to 100%) and the specificity was 69.2% (95% CI 67.8% to
70.51%), corresponding to a LR- of 0 and LR+ of 3.25.
The Sudbury Vertigo Risk Score has not been prospectively validated or validated
outside of these 3 hospitals. Additionally, the clinical utility of the score is uncertain,
as a large negative score is assigned when a diagnosis of BPPV is made (suggesting a
lack of clinical uncertainty) and a large positive score is assigned for motor/sensory
or cerebellar deficits, signs most clinicians would use to assign a central cause of
symptoms without the need for a CDR. Additionally, both the derivation and
validation studies were limited by significant differential verification bias, with only
30.9% and 36.8% of patients receiving CT scans, respectively, and only 2.5% and
5.5% undergoing MRI.